

Testosterone Therapy for Men:
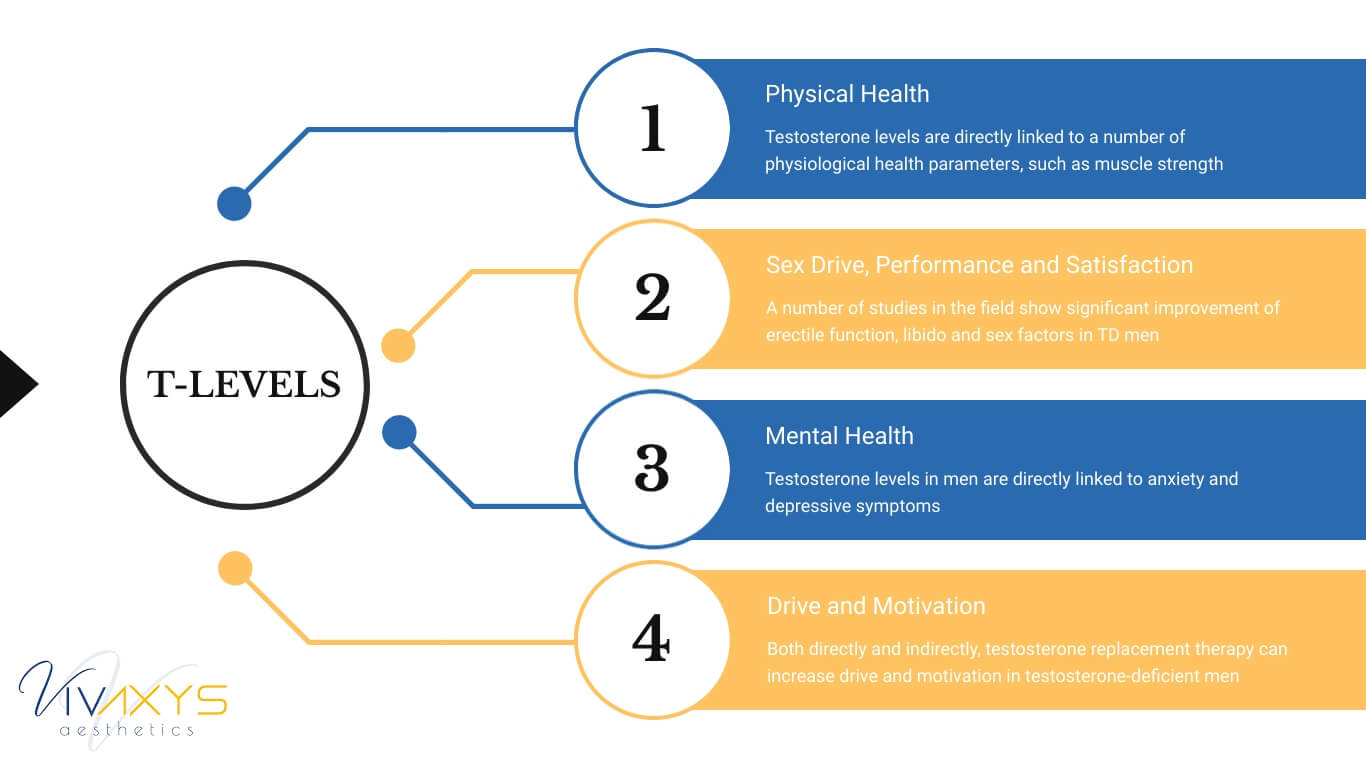
The male hormone seems to be present in all major areas of life for men. From physiological health to mental and social changes, T-levels have a major role in men’s quality of life.
What makes men, men?
Is it the physical traits? The muscle size; the bone density; the facial and body hair; low body fat percentages?
Or is it certain personal characteristics that define masculinity, such as aggressively approaching problems, being able to reach states of immense focus, and resilience towards mental problems?
Whatever your answer, somewhere during this conversation always appears one crucial actor: testosterone.
The male hormone, it seems, plays a major role in keeping men strong and healthy—both physically and mentally—as they age.
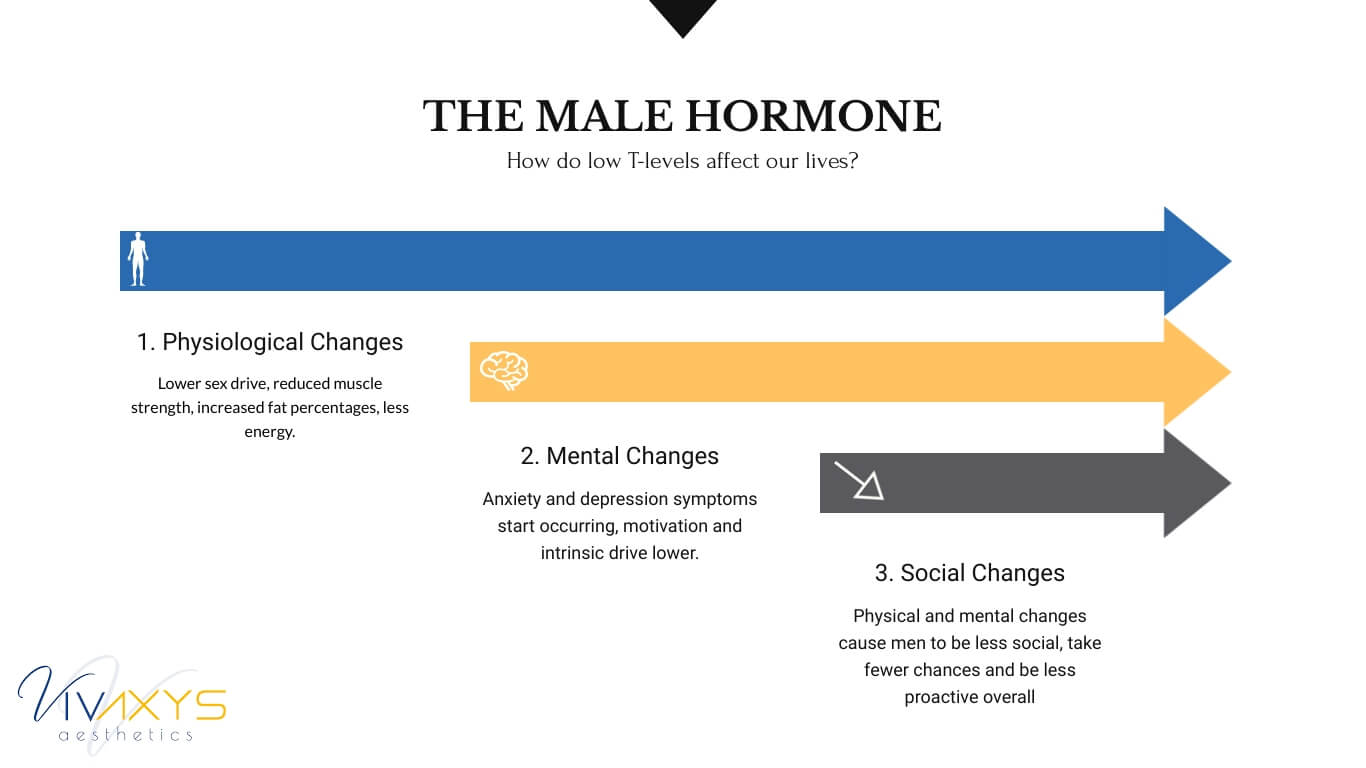
Men with low testosterone levels tend to face all sorts of physical deficiencies, from low sex drive to increased risk of cardiovascular diseases. They gain weight, lose muscle mass, become fragile, and, sometimes, even grow “man boobs.”
Mental states such as depression follow as marriages fail, along with self-confidence and self-esteem. Yellow Porsche’s and yachts don’t always seem to help.
As of today, there is no unified line of thought about what is the impact of testosterone on the male body. As in, we still don’t know for sure whether low testosterone levels are an indication of a bigger problem, or do they actually cause the problems on their own.
The best answer science can give at the moment is this: it’s both. Low testosterone levels are caused by certain conditions, but they also directly impact how well the male body functions.
What is absolutely undeniable, however, is the following fact: low testosterone levels are directly linked to a number of problems men start experiencing, usually around the 40th birthday mark.
Low testosterone treatment is still relatively new, but so is the problem itself.
Let’s not forget that the average life expectancy for white males has been less than 40 years back in 1850s—which means that the vast majority of males never reached the point where they’d start experiencing a significant drop in testosterone.
However, life expectancy more than doubled since the mid-19th century, and many men today struggle to feel like… men.
And it’s not just age that causes T-levels to drop. A number of chronic conditions plaguing the 21st century people—including diabetes and obesity—are also major contributors too.
These issues affect males deeply, in a profound way. Low sex drive for men isn’t just the tip of the iceberg: it’s the first domino piece. In many ways, it seems that Paul De Kruif, the author of testosterone manifesto, The Male Hormone, was right in concluding that “a man is as old as his testicles.”
Once their other brains go idle, men’s lives tend to enter an unstoppable downwards spiral: low libido affects marriage; marriage affects business; before you know it, it all seems to start falling apart for no apparent reason.
Unstoppable, or so it has been thought. That was before the medical frontiers moved from the physicians’ notebooks on the bedsides of the ill to the flasks and colbs of pioneer biochemists who described life in molecular formulas, not palliative advice.
But let’s start from the beginning.
What Are Hormones and What Do They Do for Us?
Hormones are the body’s chemical messengers, as described[1] by The Hormone Network. They are produced by glands, which are a part of our endocrine system.
In the simplest of terms, if our organs and cells are the “workforce” of our bodies—doing all the heavy lifting (quite literally)—then hormones are the overarching “management system” that dictates how all of our other systems behave, including the musculoskeletal and nervous systems.
Looking at the grand scheme of things, hormones are the boss: they control the algorithms that determine how our bodies allocate resources. Through that, they control our moods, physical and mental states.
Different glands produce different hormones:
- Insulin is a hormone responsible for keeping our blood sugar levels in check. Before insulin had been discovered, diabetes was considered a fatal disease. Insulin is produced in the pancreas.
- Calorie burning hormones are produced in the thyroid gland. These hormones are also responsible for keeping our heart rate within safe limits.
- The hypothalamus gland is responsible for body temperature, hunger, moods and the release of hormones from other glands; and also controls thirst, sleep and sex drive.
- Calcium, a nutrient vital for the development and strength of our bones, is developed in the parathyroid gland.
- Melatonin and its derivatives control our sleep patterns and are produced in the pineal gland.
- Lastly, testosterone is produced in our testes, and they are directly responsible for sex drive and production of sperm.
Hormones are, no more and no less, the control mechanisms of our bodies.
Low Testosterone Levels: How Do They Affect You?
If you like numbers, here are a few:
- The average man has testosterone levels around 600 ng/dl
- The upper limit of what is considered normal is around 1000 ng/dl
- Low testosterone levels are considered anything below 300 ng/dl
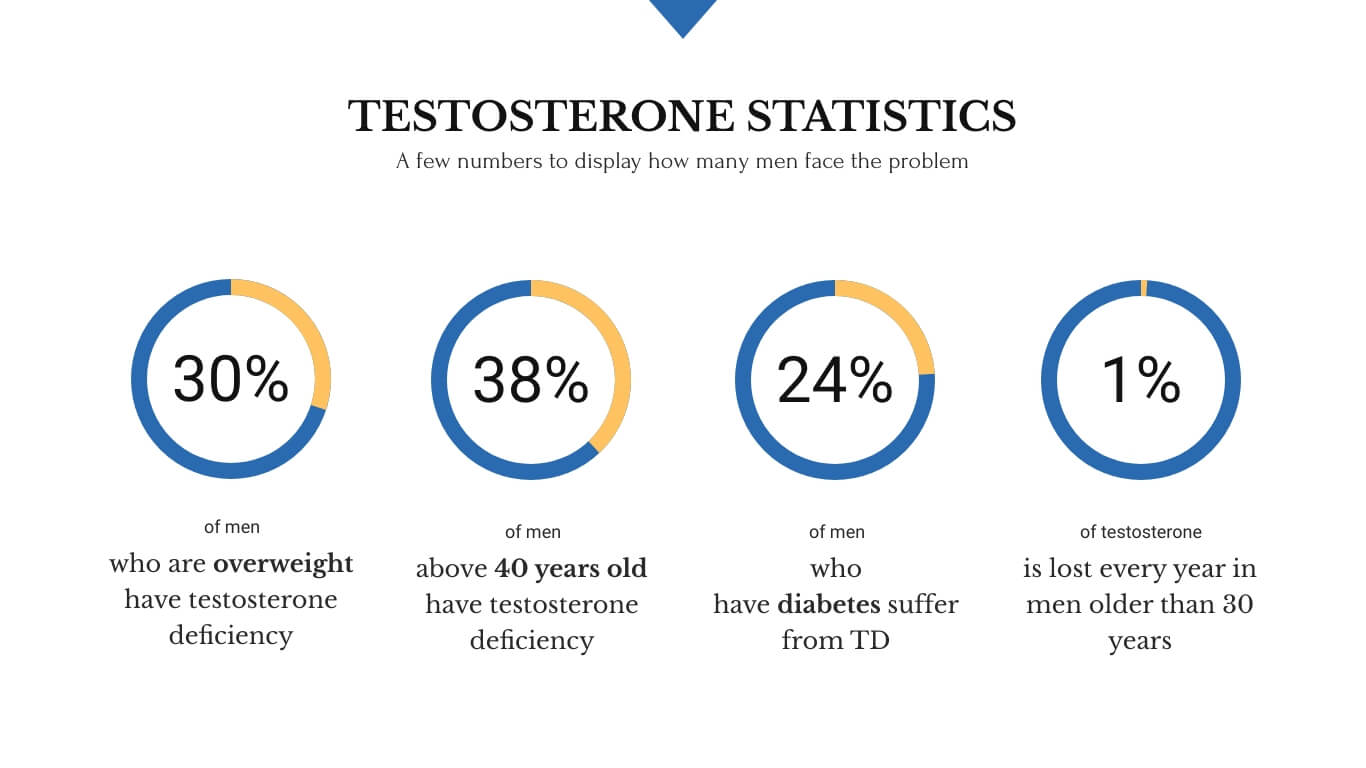
According to research, around 30% of overweight men have Testosterone Deficiency (TD.)
38% of men above 40 have testosterone levels below 300 ng/dl[2]. Above the 80-year threshold, that number spikes to 50%.
Only up to 2% of younger (read: below 30) men experience TD. However, as far as diabetes patients go, up to 24% of men have low testosterone levels.
At a normal rate, men start producing testosterone 1% less each year after hitting the 40 year-old mark.
So, what do we know about the direct effects of low testosterone levels on the male body?
In brief, we know that anything below 300 ng/dl of testosterone in the male bloodstream is directly linked to a number of symptoms. According to the Urologist Dr. Landon Trost, as the levels of testosterone decrease, more and more symptoms start showing up after a particular threshold:
- Sexual changes. As the T-levels drop in males, the sex life is usually the first line of defense. That’s where most men start seeing the symptoms, such as:
- Erectile dysfunction (ED). While low testosterone levels don’t always cause erectile problems, they are highly associated with other diseases that do cause both ED and low testosterone levels, such as diabetes, high blood pressure and high blood cholesterol levels.
- Sex drive. Surprisingly, low T-levels don’t seem to impact sex drive directly, as a major study in Massachusetts has found that only about 28% of men[3] with low testosterone experience low libido. However, testosterone deficiency significantly impacts other areas of male lives—including physical and mental health—which inevitably takes a toll on our sex lives.
- Low sperm production and infertility. While testosterone is not the only hormone responsible for healthy quantities of sperm production, it does play a crucial role.
- Physical changes. Probably the most important aspect of testosterone is its effect on men’s physical health. Low testosterone levels are directly linked to a number of health issues in men:
- Bone density. The T-hormone is directly responsible[4] for maintenance and regrowth of men’s bones. Why is this important? Well for one, diseases like osteoporosis[5] are a primary cause of morbidity and mortality in the elderly. Weakened bone structure dramatically increases the risk of fracture and chronic diseases.
- Lean muscle mass. Multiple studies arrive to the conclusion that one of testosterone’s main effects on the body have to do with muscle mass. According to this trial[6], it was concluded that testosterone significantly impacts muscle protein synthesis, which, in turn, leads to bigger, better functioning muscles.
- Body fat. It has been clinically and practically shown that testosterone levels play a direct role[7] in body composition and caloric restriction. Men with low testosterone levels tend to gain significant amounts of body fat, resulting in gynecomastia[8] (“man breasts”) and other unfavorable outcomes.
- Mental changes. Mental health in men is the last line of defence as the levels of the male hormone drop below normal. Many of mental issues are likely caused by sexual and physical changes described previously:
- Anxiety. One of the most prominent problems with low T-levels is that it causes men to lose self-confidence, causing serious anxiety problems[9]. As testosterone levels directly affect brain function[10], multiple studies have shown that men with lower testosterone are much more likely to display symptoms of chronic anxiety.
- Motivation. It is no secret that testosterone is directly linked to competition[12]. As in, the very concept of competition tends to spike testosterone levels in the competitors. Naturally, men with decreasing testosterone levels often lose the motivation to compete, whether in sports, professional lives, or other frontiers.
- Concentration and memory. While the evidence is somewhat inconsistent, it has been shown[13] that testosterone levels can have a major role in men’s ability to focus on specific tasks and memorize visual schemes.
- Depression. While by no means the only cause, multiple studies agree that the male hormone is instrumental in helping men cope with depressive symptoms[14]. There is a lot of evidence that men with higher testosterone levels—men of different age groups—are less likely to suffer from forms of depression.
Summary: testosterone affects all major parts of a man’s life, whether directly or indirectly. Scientists and practitioners are actively engaged in giving us clearer, better defined relationships between the male hormone and various bodily functions. But one thing is undeniable: testosterone plays a major role in regulating quality of life in men.
An Important Note: previously described symptoms and effects only apply to a condition called Testosterone Deficiency—blood testosterone levels below 300 dl/ng. The reverse relationships are not necessarily true—and, in many cases, aren’t—which means that more testosterone isn’t always better.
Although relatively rare, improper or excess testosterone use can lead to a number of side effects:
- Hyperthyroidism. A condition that affects the thyroid gland, which is responsible for producing metabolism-controlling hormones. Excess testosterone can cause these processes to speed up, causing increases in heart rate, sudden weight loss, significant hair loss and a number of other undesirable outcomes.
- Adrenal or testicular cancer. Improper or excessive testosterone usage can lead to certain cancerous conditions. That is why proper evaluation before the therapy is so important.
Testosterone Replacement Therapy (TRT). What Is It, Exactly?
Due to the testosterone’s numerous effects on the male psychology and physiology, treatments have emerged in the 20th century to help men maintain healthy levels of the hormone.
With the introduction of easily consumable methods of exogenous (external) testosterone—such as patches and gels—the treatment has gone mainstream in early 2000s. From year 2000 to 2011, total sales of testosterone have increased 12-fold[15].
Producing testosterone externally is no new business—and has been done since the early 20th century. The methods of administration, however, have evolved significantly for the convenience and comfort of the patients:
- Testosterone Injections

How it’s done: An oil-based solution containing testosterone is injected into the muscle. The testosterone spreads naturally into the bloodstream over time
Benefits: Cost-effective, quick, doesn’t require any preparation or post-guidance
Drawbacks: Self-injection is required, but we provide training
Available to: Anyone, except patients with history of cancer - Testosterone Patches

How it’s done: A patient places a patch on their belly, thigh or arm
Benefits: Doesn’t require going to the doctor’s office; great for long-term testosterone therapy
Drawbacks: Can irritate skin; visually unappealing; needs to be changed every 24 hours
Available to: Anyone, except patients with history of cancer - Testosterone Gel

How it’s done: A special gel is applied to the abdomen, thigh or arm area; 3-5 minutes to dry
Benefits: Doesn’t require going to the doctor’s office; great for long-term testosterone therapy
Drawbacks: Could irritate the skin; could be a slightly inaccurate dose compared to an injection, and it could rub off on your clothes
Available to: Anyone, except patients with history of cancer - Testosterone Pellets

How it’s done: The doctor will typically implant the pellets under the skin, or subcutaneously, near the hip or on the buttocks. This procedure is quick and can take place in the doctor’s office
Benefits: Testosterone pellets are a long-acting form of testosterone therapy and work by emitting a steady, low level of testosterone over a period of up to 6 months. This form of treatment is more convenient than testosterone injections and cause less skin irritation than gels or creams
Drawbacks: Minor surgical procedure is required. Risks include incorrect dosage and pellets may dislodge or come out of the skin
Available to: Anyone, except patients with history of cancer - Alternative Testosterone Administration Methods
Other ways to reinforce the male hormone exist. However, they don’t provide any obvious benefits, while increasing the risk of side effects, complications, or pure inconveniences.Testosterone implants, for example, can be surgically put into the buttocks or abdomen of a patient for long-term therapy. Many patients who have undergone testosterone implant treatment are satisfied with the results, and are more likely to continue the treatment[17], compared to patients who’ve undergone other types of testosterone administration.However, a minor surgery using a local anaesthetic is required, which can become a source of complications of its own. Also, due to the long-term, committal nature of the implant treatment, many doctors will suggest first testing the patient’s response to testosterone using non-invasive methods: if the response is positive, T-implants become a viable option.Testosterone pills are easier to consume, but they often end up being the most expensive option over time. Orally consumed testosterone is also shown to be detrimental towards the function of the liver[18], which makes it sub-optimal for long-term therapy.In general, alternative testosterone administration methods are either less effective, less convenient, more expensive, or riskier. These methods are usually recommended by doctors for patients who, for some reason, cannot undergo treatment via injections, patches and gels.
How Can Testosterone Therapy Help?
For testosterone-deficient men (T-levels below 300 ng/dl), hormone therapy can work wonders.
The direct changes are usually physiological. Men with lacking testosterone report a number of positive body changes during the treatment:
- Increased sex drive, performance and satisfaction
- Improved erectile function
- Increased muscle size and strength
- Decreased body fat percentages
- Improved bone density
These physiological effects make men feel younger, more energetic—more themselves—once again.

The improvement naturally leads to better mental states. While direct effects of testosterone on quality of life are still being studied, it is evident that testosterone therapy can:
- Reduce anxiety
- Reduce depressive symptoms
- Improve sexual and other relationships
- Restore self-confidence
- Increase motivation and professional drive
In other words, once men start feeling like men again, everything starts falling into place.
Who Is a Good Candidate for Testosterone Therapy?
The first thing that you’ll be tested for is—big surprise—the level of testosterone in your bloodstream.
Why? Because testosterone therapy doesn’t work both ways. If you have below-normal T-levels, then a testosterone replacement therapy might do wonders for you. However, once you hit regular hormone levels, there’s no obvious benefit to adding more testosterone into your system.
To put it in the simplest of terms: if you have normal testosterone levels, adding more of the hormone likely won’t give you bigger muscles or larger sex drive.
While there are several different tests conducted in the lab, what you need to know is that a sample of your blood will be taken to evaluate current T-levels in your system.
Before the blood test, it is advisable to avoid certain medications, such as steroids[19], anticonvulsants[20] (anti-seizure medication), barbiturates[21] and clomiphene[22]. Your doctor will provide detailed guidelines on which medications and supplements to avoid specifically before the test.
If the levels of testosterone are indeed low, you will be more closely evaluated for testosterone therapy.

Men with the following conditions are usually dissuaded from testosterone therapy, as TRT can actually make these conditions worse:
- Untreated heart problems
- Sleep apnea
- History of increased quantity of red blood cells
What about fertility?
It is true that TRT may affect your sperm count and fertility. That’s why people who are planning on having children are heavily forewarned of this danger. Coincidentally, most TRT patients do not intent on conceiving in the nearest future and have other concerns.
Is Testosterone Therapy Safe? Are There Any Side Effects?
In general, testosterone therapy is a safe option for the right candidate
There are a few common side effects that are related to various methods of testosterone administration that patients can experience during the treatment.
For example, some testosterone patch users experience skin irritation and redness in the treatment area. It is a common side effect associated with T-patches.
Testosterone injections can also cause mild reactions from your body. Some patients report increased acne, accelerated body hair growth and, sometimes, even occasional nausea.
However, there are a few things for you to keep in mind before you consider these side effects:
- Most of the heavy lifting is done before the treatment is ever begun. Your doctor’s evaluation whether you’re a good TRT candidate will prove to be the most significant factor in whether you experience any side effects or not. After evaluating a range of factors, your doctor will tailor the treatment plan to make your treatment as smooth as possible.
- TRT is an ongoing process, and there’s always time to readjust. It is a mistake to think that TRT is a one-time treatment. Due to its extensive, ongoing nature, your doctor will regularly monitor your body functions and see if any of the symptoms occur. Once there are first signs of the side effects, adjustments can be made to the treatment plan.
- There are always options available. With TRT, there is no one-size-fits-all type of solution. Luckily, there are a myriad of ways to administer the hormone into the patient’s body, from patches to injections to pills. Dosages can also be adjusted based on the patient’s body response to the treatment.
One of the more common concerns we receive about TRT are in regards to the treatment’s effects on fertility.
While there is evidence that exogenous testosterone administration can diminish a man’s natural ability to produce sperm, there are a couple of important things to consider:
- There are proven therapy methods than can effectively negate the “infertility effect” of testosterone therapy
- Most men with low-testosterone levels are at an age where they aren’t actively considering children
Does Testosterone Replacement Therapy (TRT) Work?
Naturally, the most important thing is whether TRT actually works in real-life settings.
The short answer is this: it does.
For the right candidates, thousands of trials have shown to significantly improve:
- Muscle mass and function. Men with low testosterone levels experience a tremendous increase in chest, leg and arm muscle size and strength. The changes occur relatively soon after the start of the treatment – in some cases, performance peaked at 90 days.
- Sex drive and function. One of the primary reasons to consider TRT, hormone administrations show incredible improvement in the patients’ sex lives. Testosterone injections, gels and patches have been repeatedly shown to improve erectile function, libido, sexual performance and satisfaction.
- Body fat and composition. Hundreds of trials have successfully displayed that exogenous testosterone results in a significant increase in lean body weight and a reduction in overall fat percentages.
Here’s more information about those trials.
TRT Effects on Lean Muscle Mass and Power
A number of studies show positive effects of exogenous testosterone administration on the patients’ muscle mass and function:
- In a trial of 61 men between ages 18 and 31, a significant increase[23] was observed in leg press strength, thigh, and quadriceps muscle volume after administering monthly doses of testosterone
- Another 2009 study[24] of 122 men aged from around 65 to 75 observed a two-fold increase in lean muscle mass (on average) and a significant reduction in overall body fat as well as increased aerobic ability, strength and endurance among all patient groups after a 16 week testosterone treatment
- The same year, a trial of seventy men[25] with median age of 70 were randomly assigned to take testosterone injections every 6 weeks. Isometric strength and peak torque in the quadriceps has improved significantly in the test group.
More similar studies regarding muscle mass and power:
- “Changes in muscle mass, muscle strength, and power but not physical function are related to testosterone dose in healthy older men.”, 2008 (Link[26])
Trial subjects: 60, healthy, community-dwelling men, aged 60 to 75
Treatment: Monthly testosterone injections, intramuscular, for 20 weeks
Results: Maximum muscle strength increased, leg power increased significantly - “Transdermal testosterone gel improves sexual function, mood, muscle strength, and body composition parameters in hypogonadal men”, 2000 (Link[27])
Trial subjects: 227 hypogonadal (testosterone-deficient) men
Treatment: Transdermal T-gel, 50-100 mg of testosterone daily, for 180 days
Results: Mean muscle strength in the leg press exercise increased by 11 to 13 kg in all treatment groups by 90 days, moderate increases in arm/chest muscle size, significant increases in lean body mass in all patient groups - “Effects of testosterone on muscle strength, physical function, body composition, and quality of life in intermediate-frail and frail elderly men: a randomized, double-blind, placebo-controlled study”, 2010 (Link[28])
Trial subjects: 274 community-dwelling men, at least 65 years old
Treatment: Transdermal T-gel, 50 mg of testosterone daily, for 6 months
Results: Knee extension peak torque improved significantly, lean body mass increased, fat percentage decreased, physical function improved in the test group
Summary: TRT Effects on Muscle Size and Power
Looking at the big picture, studies tell us that:
- Testosterone therapy has a number of positive effects on muscle mass, size and function in testosterone-deficient men of all age groups
- Most significant effects on muscle size and function can be observed within 12-20 from the start of the treatment
- Larger testosterone doses tend to result in bigger muscle gains for men with low testosterone levels
TRT Effects on Fat and Body Composition
Testosterone levels play a major role[29] in fat percentages and overall body composition. Testosterone replacement therapy has been shown to significantly impact body composition in obese patients:
- During the previously mentioned 180-day study[30] of 227 testosterone-deficient men, it has been shown that patient groups ongoing T-gel treatment have lost 1 kg of fat mass (on average), while lean body mass increased by 2.7 kg (on average) after 90 days of daily treatment
- An older study of 13 healthy men[31], 57-76 yr old with “borderline low” testosterone levels showed that hormone injections have a positive impact on the patients’ lean body mass and lowers cholesterol levels
- A number of studies have shown a significant decrease in total weight in testosterone-deficient men on therapy after 3 months[32], 6 months[33] and 24 months[34] into the treatment and significantly lower fat percentages after 3 months[35]
TRT Effects on Sex Drive and Erectile Function
One of the main appeals behind testosterone therapy remains its ability to restore libido in testosterone-deficient men. A number of studies show positive effect on sex drive and ability in response to treatment:
- Research shows that testosterone administration has a much more rapid effect on sexual parameters. Studies show dramatic improvement in “libido, sexual desire, sexual thoughts and fantasies and satisfaction with sexual life” occur as soon as 3 weeks[36] into the treatment
- 3 weeks is also the time frame for testosterone to take effect on a patient’s erection, with some changes occurring as soon as 30 days after the initial treatment[37]. Patients report more frequent erections, better sexual performance and satisfaction.
- For patients with veno-occlusive dysfunction, the changes take longer to manifest: in a 2006 study[38] of 12 men with low testosterone levels and erectile dysfunction, the treatment took from 3 to 11 months to show significant improvement
Key Takeaways: What You Need to Know about TRT
- TRT isn’t a source of eternal youth for everyone, but it can help the right candidates restore their body function to normal levels
- TRT is only effective for men with low testosterone levels (<300 ng/dl). For men with normal T-levels, there is no obvious benefit with the therapy
- Multiple TRT studies show that sexual function improves dramatically within 30 days of treatment, while muscle mass, strength and body composition manifest fully within a 2-12 month period
- TRT is safe for the right candidate, but a close examination by a qualified doctor is necessary to evaluate. For patients with certain health conditions and under certain medications, TRT can make things worse
- Testosterone can be administered in a number of ways based on the patient’s preferences and body reactions, including patches, gels, injections, and pills
References
1. “Hormones” by The Hormone Network. Source:
https://www.hormone.org/hormones-and-health/hormones
2. McBride JA, Coward RM. Recovery of spermatogenesis following testosterone replacement therapy or anabolic-androgenic steroid use. Asian J Androl. 2016;18(3):373-80. Source:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4854084/
3. “Low Testosterone and Sex Drive” by WebMD. Source:
https://www.webmd.com/men/how-low-testosterone-can-affect-your-sex-drive#1
4. Tyagi V, Scordo M, Yoon RS, Liporace FA, Greene LW. Revisiting the role of testosterone: Are we missing something?. Rev Urol. 2017;19(1):16-24. Source:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5434832/
5. “Osteoporosis” by National Institute on Aging. Source:
https://www.nia.nih.gov/health/osteoporosis
6. Griggs RC, Kingston W, Jozefowicz RF, Herr BE, Forbes G, Halliday D. Effect of
testosterone on muscle mass and muscle protein synthesis. J Appl Physiol (1985).
1989 Jan;66(1):498-503. PubMed PMID: 2917954. Source:
https://www.ncbi.nlm.nih.gov/pubmed/2917954
7. Ng Tang Fui M, Prendergast LA, Dupuis P, et al. Effects of testosterone treatment on body fat and lean mass in obese men on a hypocaloric diet: a randomised controlled trial. BMC Med. 2016;14(1):153. Published 2016 Oct 7. doi:10.1186/s12916-016-0700-9. Source:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5054608/
8. “Enlarged breasts in men (gynecomastia)” by Mayo Clinic. Source:
https://www.mayoclinic.org/diseases-conditions/gynecomastia/symptoms-causes/syc-20351793
9. Berglund LH, Prytz HS, Perski A, Svartberg J. Testosterone levels and
psychological health status in men from a general population: the Tromsø study.
Aging Male. 2011 Mar;14(1):37-41. doi: 10.3109/13685538.2010.522276. Epub 2010
Oct 5. PubMed PMID: 20923289. Source:
https://www.ncbi.nlm.nih.gov/pubmed/20923289
10. Domonkos E, Hodosy J, Ostatníková D, Celec P. On the Role of Testosterone in
Anxiety-Like Behavior Across Life in Experimental Rodents. Front Endocrinol
(Lausanne). 2018 Aug 6;9:441. doi: 10.3389/fendo.2018.00441. eCollection 2018.
Review. PubMed PMID: 30127767; PubMed Central PMCID: PMC6088149. Source:
https://www.ncbi.nlm.nih.gov/pubmed/30127767
12. Casto KV, Edwards DA. Testosterone, cortisol, and human competition. Horm
Behav. 2016 Jun;82:21-37. doi: 10.1016/j.yhbeh.2016.04.004. Epub 2016 Apr 19.
Review. PubMed PMID: 27103058. Source:
https://www.ncbi.nlm.nih.gov/pubmed/27103058
13. Celec P, Ostatníková D, Hodosy J. On the effects of testosterone on brain behavioral functions. Front Neurosci. 2015;9:12. Published 2015 Feb 17. doi:10.3389/fnins.2015.00012. Source:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4330791/
14. Celec P, Ostatníková D, Hodosy J. On the effects of testosterone on brain behavioral functions. Front Neurosci. 2015;9:12. Published 2015 Feb 17. doi:10.3389/fnins.2015.00012. Source:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4330791/
15. Sheahan, William T et al. “Testosterone Replacement Therapy: Playing Catch-up With Patients” Federal practitioner : for the health care professionals of the VA, DoD, and PHS vol. 32,6 (2015): 26-31. Source:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6363308/
16. “Testogel” by Virtual Medical Centre. Source: https://www.myvmc.com/drugs/testogel/
17. “Testosterone Replacement Therapy in Men” by Virtual Medical Centre. Source:
https://www.myvmc.com/treatments/testosterone-replacement-therapy-in-men
18. Almaiman AA. Effect of testosterone boosters on body functions: Case report. Int J Health Sci (Qassim). 2018;12(2):86-90. Source:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5870326/
19. “Bulk Up Your Steroid Smarts” by WebMD. Source:
https://www.webmd.com/a-to-z-guides/ss/slideshow-steroids-101
20. “Anticonvulsant/Anti-Seizure Medication from A to Z” by Epilepsy Ontario. Source:
http://epilepsyontario.org/about-epilepsy/treatments/medications/anticonvulsantanti-seizure-medication-from-a-to-z/
21. “Barbiturates” by RxList. Source:
https://www.rxlist.com/consumer_barbiturates/drugs-condition.htm
22. “Clomiphene” by MedlinePlus. Source:
https://medlineplus.gov/druginfo/meds/a682704.html
23. Bhasin S, Woodhouse L, Casaburi R, Singh AB, Bhasin D, Berman N, Chen X,
Yarasheski KE, Magliano L, Dzekov C, Dzekov J, Bross R, Phillips J, Sinha-Hikim
I, Shen R, Storer TW. Testosterone dose-response relationships in healthy young
men. Am J Physiol Endocrinol Metab. 2001 Dec;281(6):E1172-81. Source:
https://www.ncbi.nlm.nih.gov/pubmed/11701431
24. Sattler FR, Castaneda-Sceppa C, Binder EF, Schroeder ET, Wang Y, Bhasin S,
Kawakubo M, Stewart Y, Yarasheski KE, Ulloor J, Colletti P, Roubenoff R, Azen SP.
Testosterone and growth hormone improve body composition and muscle performance
in older men. J Clin Endocrinol Metab. 2009 Jun;94(6):1991-2001. doi:
10.1210/jc.2008-2338. Epub 2009 Mar 17. PubMed PMID: 19293261; PubMed Central
PMCID: PMC2690426. Source:
https://www.ncbi.nlm.nih.gov/pubmed/19293261
25. Caminiti G, Volterrani M, Iellamo F, Marazzi G, Massaro R, Miceli M, Mammi C,
Piepoli M, Fini M, Rosano GM. Effect of long-acting testosterone treatment on
functional exercise capacity, skeletal muscle performance, insulin resistance,
and baroreflex sensitivity in elderly patients with chronic heart failure a
double-blind, placebo-controlled, randomized study. J Am Coll Cardiol. 2009 Sep
1;54(10):919-27. doi: 10.1016/j.jacc.2009.04.078. PubMed PMID: 19712802. Source:
https://www.ncbi.nlm.nih.gov/pubmed/19712802
26. Storer TW, Woodhouse L, Magliano L, Singh AB, Dzekov C, Dzekov J, Bhasin S.
Changes in muscle mass, muscle strength, and power but not physical function are
related to testosterone dose in healthy older men. J Am Geriatr Soc. 2008
Nov;56(11):1991-9. doi: 10.1111/j.1532-5415.2008.01927.x. Epub 2008 Sep 15.
PubMed PMID: 18795988; PubMed Central PMCID: PMC2585153. Source:
https://www.ncbi.nlm.nih.gov/pubmed/18795988
27. Wang C, Swerdloff RS, Iranmanesh A, Dobs A, Snyder PJ, Cunningham G, Matsumoto
AM, Weber T, Berman N; Testosterone Gel Study Group. Transdermal testosterone gel
improves sexual function, mood, muscle strength, and body composition parameters
in hypogonadal men. J Clin Endocrinol Metab. 2000 Aug;85(8):2839-53. PubMed PMID:
Source:
https://www.ncbi.nlm.nih.gov/pubmed/10946892
28. Srinivas-Shankar U, Roberts SA, Connolly MJ, O’Connell MD, Adams JE, Oldham
JA, Wu FC. Effects of testosterone on muscle strength, physical function, body
composition, and quality of life in intermediate-frail and frail elderly men: a
randomized, double-blind, placebo-controlled study. J Clin Endocrinol Metab. 2010
Feb;95(2):639-50. doi: 10.1210/jc.2009-1251. Epub 2010 Jan 8. PubMed PMID:
Source:
https://www.ncbi.nlm.nih.gov/pubmed/20061435
29. Allan CA, McLachlan RI. Androgens and obesity. Curr Opin Endocrinol Diabetes
Obes. 2010 Jun;17(3):224-32. doi: 10.1097/MED.0b013e3283398ee2. Review. PubMed
PMID: 20418719. Source:
https://www.ncbi.nlm.nih.gov/pubmed/20418719
30. Tenover JS. Effects of testosterone supplementation in the aging male. J Clin
Endocrinol Metab. 1992 Oct;75(4):1092-8. PubMed PMID: 1400877. Source:
https://www.ncbi.nlm.nih.gov/pubmed/1400877
31. Boyanov MA, Boneva Z, Christov VG. Testosterone supplementation in men with
type 2 diabetes, visceral obesity and partial androgen deficiency. Aging Male.
2003 Mar;6(1):1-7. PubMed PMID: 12809074. Source:
https://www.ncbi.nlm.nih.gov/pubmed/12809074
32. Page ST, Amory JK, Bowman FD, Anawalt BD, Matsumoto AM, Bremner WJ, Tenover
JL. Exogenous testosterone (T) alone or with finasteride increases physical
performance, grip strength, and lean body mass in older men with low serum T. J
Clin Endocrinol Metab. 2005 Mar;90(3):1502-10. Epub 2004 Nov 30. Source:
https://www.ncbi.nlm.nih.gov/pubmed/15572415
33. Haider A, Gooren LJ, Padungtod P, Saad F. Improvement of the metabolic
syndrome and of non-alcoholic liver steatosis upon treatment of hypogonadal
elderly men with parenteral testosterone undecanoate. Exp Clin Endocrinol
Diabetes. 2010 Mar;118(3):167-71. doi: 10.1055/s-0029-1202774. Epub 2009 May 26.
PubMed PMID: 19472103. Source:
https://www.ncbi.nlm.nih.gov/pubmed/19472103
34. Boyanov MA, Boneva Z, Christov VG. Testosterone supplementation in men with
type 2 diabetes, visceral obesity and partial androgen deficiency. Aging Male.
2003 Mar;6(1):1-7. PubMed PMID: 12809074. Source:
https://www.ncbi.nlm.nih.gov/pubmed/12809074
35. Jockenhövel F, Minnemann T, Schubert M, Freude S, Hübler D, Schumann C,
Christoph A, Gooren L, Ernst M. Timetable of effects of testosterone
administration to hypogonadal men on variables of sex and mood. Aging Male. 2009
Dec;12(4):113-8. doi: 10.3109/13685530903322858. PubMed PMID: 19909203. Source:
https://www.ncbi.nlm.nih.gov/pubmed/19909203
36. Jockenhövel F, Minnemann T, Schubert M, Freude S, Hübler D, Schumann C,
Christoph A, Gooren L, Ernst M. Timetable of effects of testosterone
administration to hypogonadal men on variables of sex and mood. Aging Male. 2009
Dec;12(4):113-8. doi: 10.3109/13685530903322858. PubMed PMID: 19909203. Source:
https://www.ncbi.nlm.nih.gov/pubmed/19909203
37. Yassin AA, Saad F, Traish A. Testosterone undecanoate restores erectile
function in a subset of patients with venous leakage: a series of case reports. J
Sex Med. 2006 Jul;3(4):727-735. doi: 10.1111/j.1743-6109.2006.00267.x. PubMed
PMID: 16839330. Source:
https://www.ncbi.nlm.nih.gov/pubmed/16839330

